The proximal portion of the tendon of the long head of the biceps is situated inside the joint and is within the synovial membrane of the glenohumeral joint. This tendon goes distally through the bicipital groove formed between the lesser tuberosity and greater tuberosity respectively located on the anterior and lateral portions of the head of the humerus.
The synovial sheath of the glenohumeral joint continues 3-4cm distally to the inferior extremity of the bicipital groove and makes contact with the sheath of the long biceps. This proximity explains the frequent relation between the symptoms/affections of the tendon of the long biceps and the glenohumeral joint.
The tendon of the long biceps has a curvilinear path du to its origin situated medially relatively to its muscle belly. Because of this path the tendon has an inherent tendency to move towards the midline, especially during a powerful contraction. The transverse humeral ligament covers the bicipital groove forming a osteofibrous channel that reduces the likelihood of the tendon to move medially.
The rotator interval is the name given to the space separating the subscapular tendon and the supraspinatus tendon. It contains the tendon of the long biceps, the coracohumeral ligament and the superior glenohumeral ligament. These structures work together to maintain the tendon of the long biceps in place within the bicipital groove.
Unlike its counterpart, the tendon of the short biceps reaches its origin without going through the glenohumeral articulation and is thus rarely involved in shoulder disorders (Bianchi, 2007).
The subacromial space is delimited by the coracoacromial arch and the head of the humerus. This space contains the tendons of the rotator cuff, the tendon of the long biceps and the subacromial-subdeltoid bursa
The tendon of the long biceps is located in the bicipital groove
The bicipital groove is between the the lesser tuberosity and greater tuberosity respectively located on the anterior and lateral portions of the head of the humerus
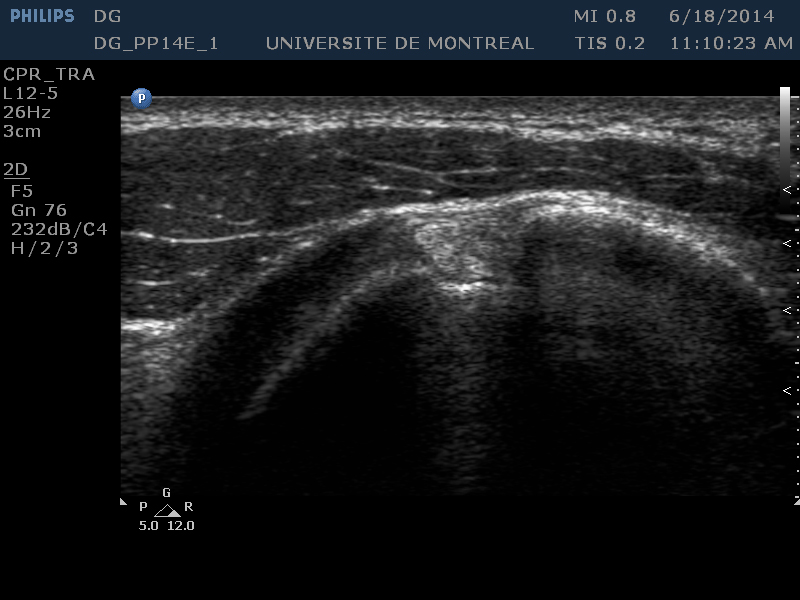
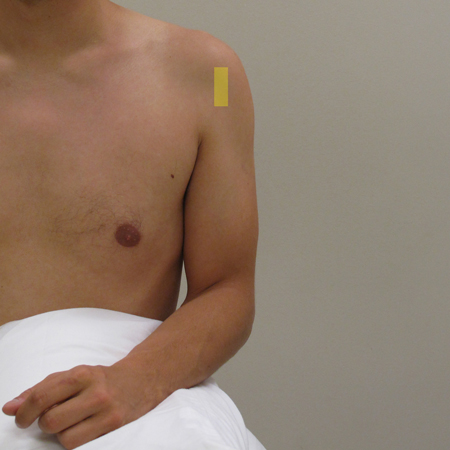
Place the probe in transverse plane at the bicipital groove
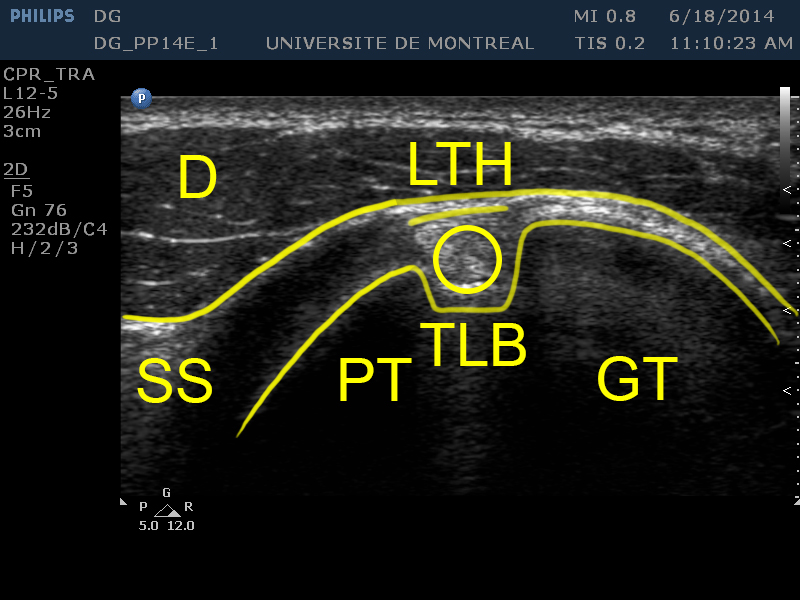
Identifying structures (on the screen) :
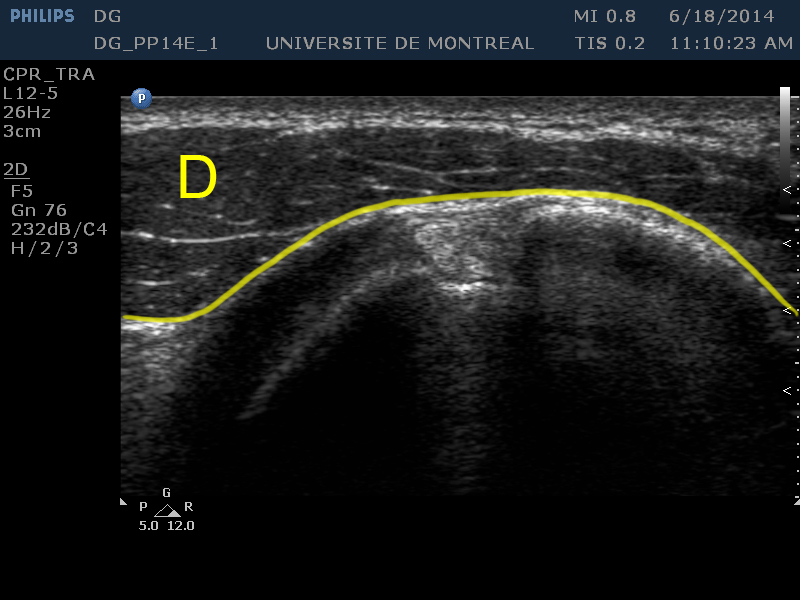
[D]
The deltoid appears at the top of the image
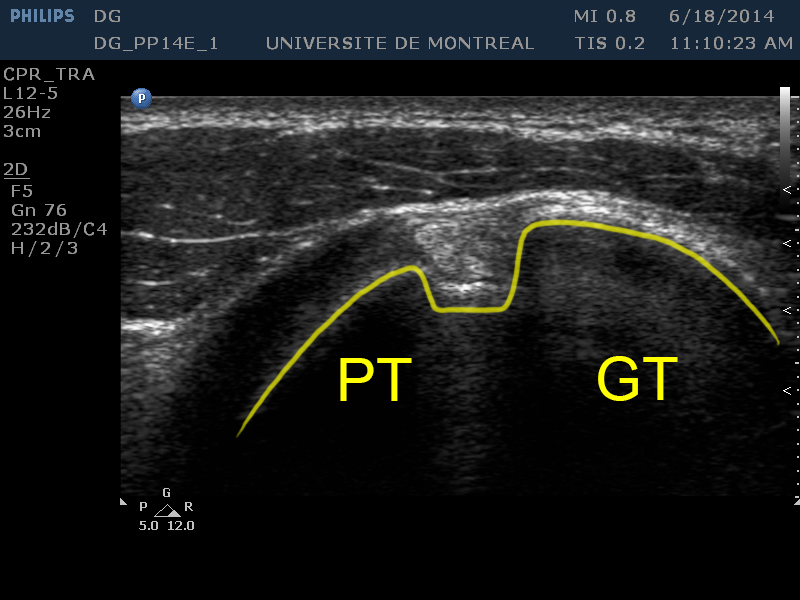
[LT] [GT]
The lesser tuberosity and greater tuberosity (circular hypoechoic zone of the humeral head) occupy the central portion of the screen respectively on the left and on the right of the image.
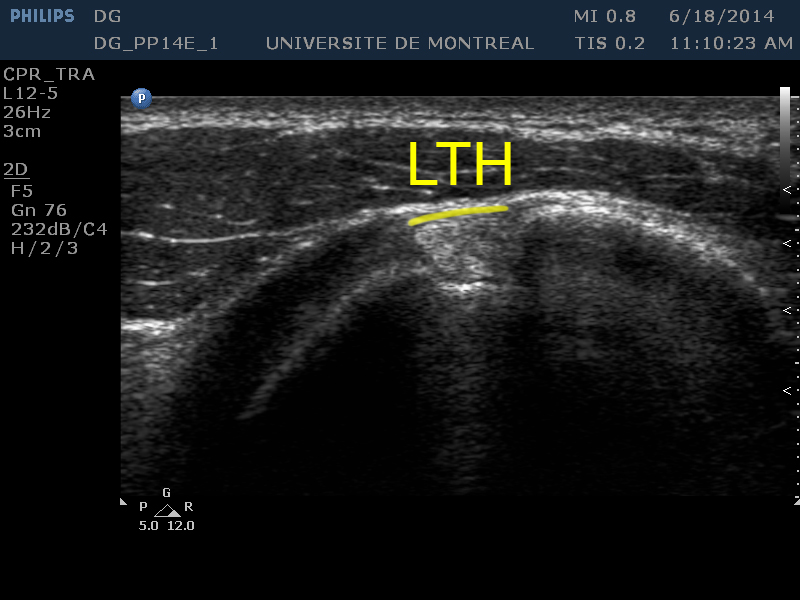
[THL]
The transverse humeral ligament (thin hypoechoic layer) forms the top part of the osteofibrous channel that is the bicipital groove.
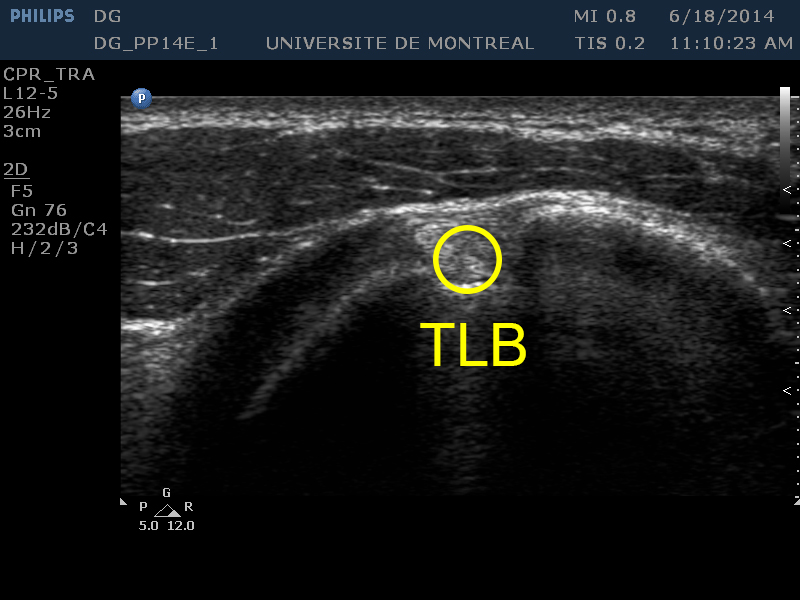
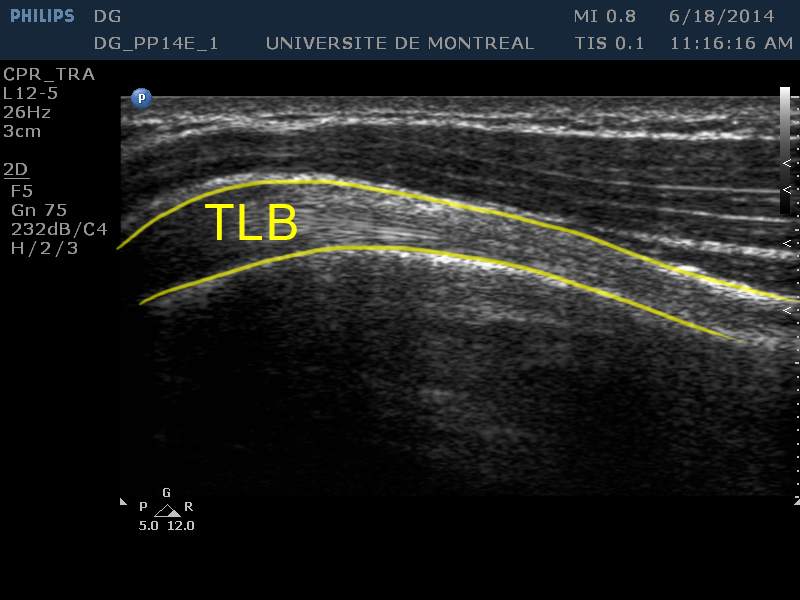
[TLB]
The tendon of the long biceps is visible within the bicipital groove.
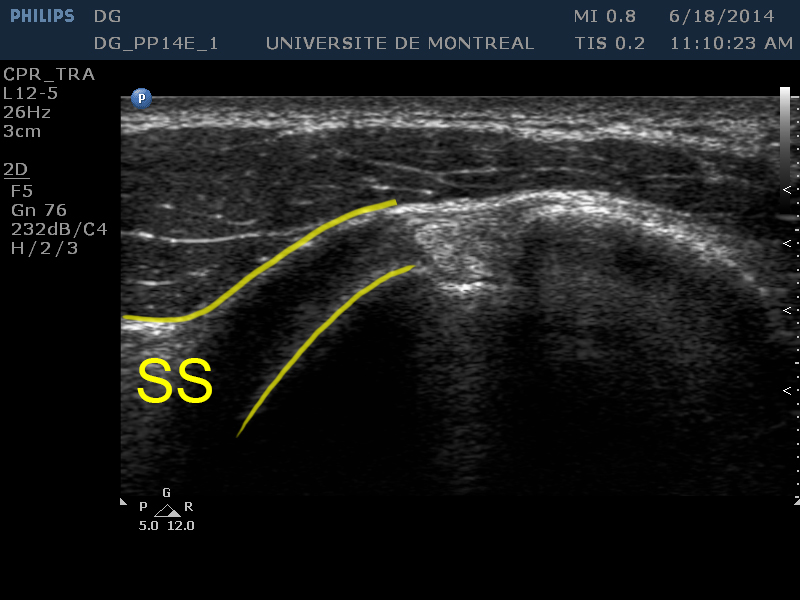
[SS]
The subscapular tendon is visible on the left of the image above the lesser tuberosity.
The intra-articular portion of the tendon of the long biceps can demonstrate the presence of effusion in the tendon sheath
This sign suggests a tendinopathy of the biceps brachii but is not suffisant to make a diagnosis
Tendinosis by attrition over an irregular bone
Identify longitudinal separations
Be careful not to confuse with a bifurcated tendon (anatomical variant)
Suspected rupture
Identify a discontinuity in the tendon of the long biceps
Useful when the clinical evaluation is complex (ex. obese patients)
Suspected impingement
Identify a impingement within the acromiohumeral space
Using a dynamic application
Observation of the subluxation of the tendon of the long head from the bicipital groove
Identify the sliding mouvement (snapping) of the tendon of the long biceps. It often occurs during a simultaneous abduction and internal rotation of the shoulder