The subscapular muscle is mainly situated on the anterior face of the shoulder. It is one of the four muscles that make up the rotator cuff with the supraspinatus (superior face), the infraspinatus and the teres minor (both on the posterior face). The subscapular originates on the front side of the scapula, an area named subscapular fossa. The subscapular is composed of two or three muscle bellies which unite to form a subscapular tendon that inserts on the lesser tuberosity of the humerus.
Due to its depth, the subscapularis is the only muscle of the rotator cuff which cannot be properly or efficiently palpated. During the ultrasonographic evaluation, it is necessary to position the shoulder in external rotation in order to evaluate the proximal tendon of the subscapularis. This approach allows to stretch the subscapular muscle and free it from the coracoid process which normally covers part of it. We can therefore benefit from a more superficial access to the muscle for the ultrasound beam.
Because of the axis of its tendon, the subscapular muscle is a powerful internal rotator and adductor of the glenohumeral joint.
Once the bicipital groove is located, position the shoulder in external rotation while ensuring not to induce a flexion/abduction. (keep the elbow on the iliac crest)
Place the probe in a longitudinal orientation at the bicipital groove
Sweep the probe up and down to cover the entire area of the subscapular muscle and its tendon. These structures cover an area larger then the size of the probe.
Identifying structures (on the screen) :
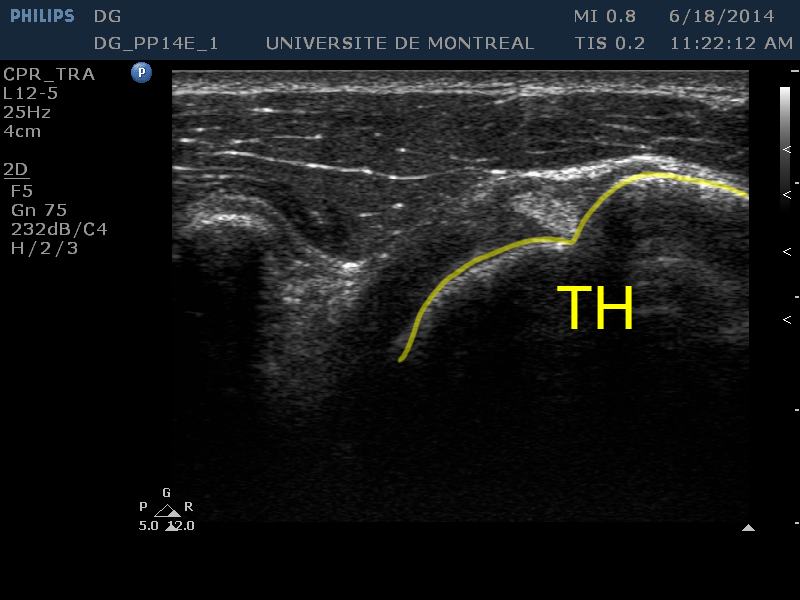
[HH]
The humeral head, large circular hypoechoic zone, appears on the right of the image.
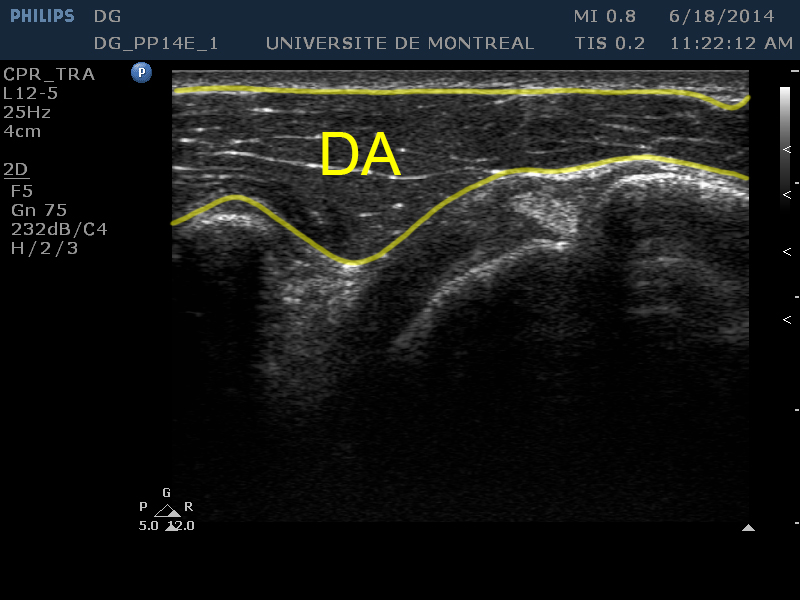
[AD]
The anterior deltoid is a thick layer, slightly hyperechoic relatively to the humeral head. It is visible on the superior part of the image.
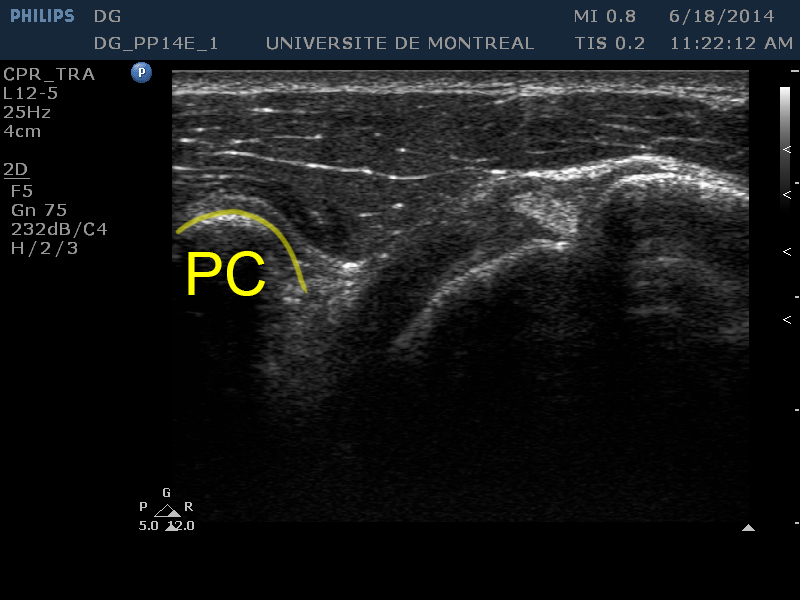
[CP]
The coracoid process, a part of the scapula, is located on the left of the image. We can also see a shady area (artefact) under this structure.
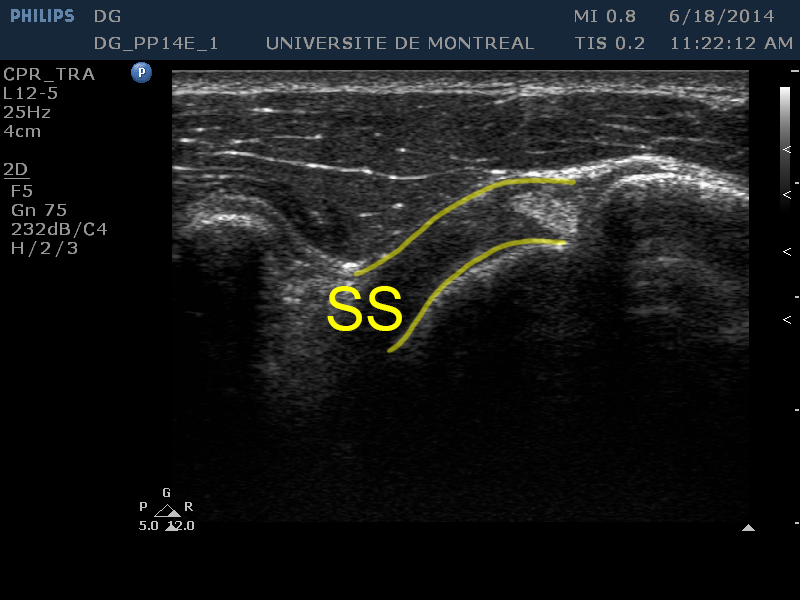
[SS]
The subscapularis tendon can be observed between the anterior deltoid and the humeral head. It has similar echogenic properties as muscle tissu but its echotexture is more smooth and homogeneous.
Evaluation of the multipennate structure of the subscapularis
Suggested settings :
Depth : 3-4 cm
Gain : 70-74
F/1/3
Probe position :
Turn the probe 90° relative to the longitudinal plane
Identifying structures (on the screen) :
[PMa]
The pectoralis major appears at the top of the image as a thick hypoechoic layer.
[PMi]
The pectoralis minor appears on the right of the image as a triangular hypoechoic layer.
[SS]
The subscapularis is located under the pectoralis major. The echogenicity is mixed but hyperechoic relative to the pectoralis major.
[MP]
The multipennate structure is visible in the frame and appears as alternating hyper and hypoechoic lines. These lines are respectively tendon and muscle tissu.
An isolated rupture of the subscapularis tendon is rare. When the occur, they are mostly located at the subscapularis insertion on the lesser tuberosity (Bianchi, p.216).
A significant retraction of the tendon following a complete rupture is common. This retraction becomes even more evident when the shoulder is placed in external rotation (Jacobson, p.66).
During the transverse evaluation of the subscapularis, it is important not to confuse the multipennate structure (alternating hypo and hyperechoic zones) with a rupture (Bianchi, p.214).
Complete ruptures of the subscapularis tendon are frequently accompanied by the dislocation of the long bicep tendon. The long bicep tendon is then repositioned within the glenohumeral joint.
When the rupture of the subscapularis tendon is incomplete and mainly located at the cranial fibers (superior) it can be accompanied by the rupture of the anterior portion of the supraspinatus and even rupture of the rotator cuff in all its thickness (Jacobson, p.66).
In this type of rupture, the tendon of the long biceps normally tends to move above the lesser tuberosity.