The supraspinatus muscle is located on the posterosuperior region of the shoulder. It is one of the four muscles that make up the rotator cuff with the subscapularis (anterior region), the infraspinous and the teres minor (posterior region). The supraspinatus origins at the supraspinous fossa whose name refers to the spine of the scapula. Its insertion is located at the superior portion of the greater tuberosity of the humeral head. The supraspinatus has one muscle belly and one origin-insertion axis (when in anatomical position) oriented towards from interior to exterior, from front to back and from top to bottom. Because of its axis, this muscle is involved in external rotation (mainly) and abduction of the glenohumeral joint. When undertaking an ultrasonographic exam, good knowledge of the orientation of each muscle is essential.
The intra-articular portion of the long biceps is a good starting point to visualize the path of the supraspinatus muscle. Both tendons are parallel (in this area) and the tendon of the long biceps has a very characteristic echotexture and echogenicity that make it a very recognizable reference point.
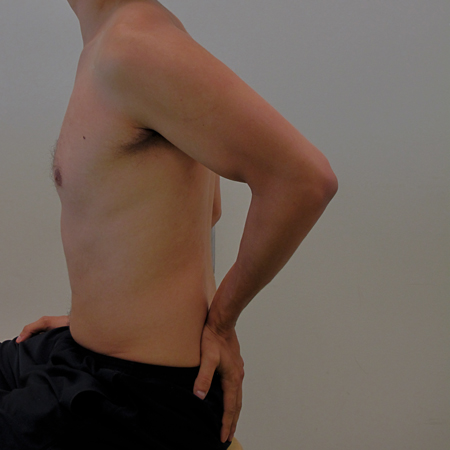
When the shoulder is placed in resting position, only the distal portion of the supraspinal tendon is visible for examination. The reste of the tendon is hidden by the acromioclavicular arch and the humeral head. As part of an ultrasonographic evaluation, the patient is often asked to adopt a position that will place the supraspinatus more anteriorly giving acces to the tendon and the musculotendinous junction.
The distal third of the supraspinatus muscle passes in the subacromial space just before its distal musculotendinous junction. The subacromial space is delimited by the coracoacromial arch and the humeral head. This space contains the tendons of the rotator cuff muscles and the long biceps. It also contains the subacromial and subdeltoid bursa. The volume of this space varies from one individual to the other due to several factors including :
A well documented anatomical variability ;
The shoulder position (neutral vs rotation / flexion / abduction) ;
Age (possible degenerative components) ;
The potential presence of various shoulder injuries and disorders
This anatomical variability is often subject to a classification that recognizes three types of acromion: flat (type I, 4.7% of the population); curved (type II 51.76% of the population); hooked (type III 43.52% of the population). There is also an interesting correlation between the acromion morphologies (as described above) and the incidence of complete rotator cuff tears. This correlation based on the evaluation of 140 shoulders in study by Bigliani et al is summarized in table below.
Acromial types
Incidence of complete rotator cuff tears
Type I (flat)
3,0 %
Type II (curved)
24,2 %
Type III (hooked)
69,8%
Several other mesures and classifications existe to describe the different morphologies of the acromion and subacromial space including the acromion index (AI), the lateral acromial angle (LAA), the critical shoulder angle (CSA) and the acromial slope (AS).
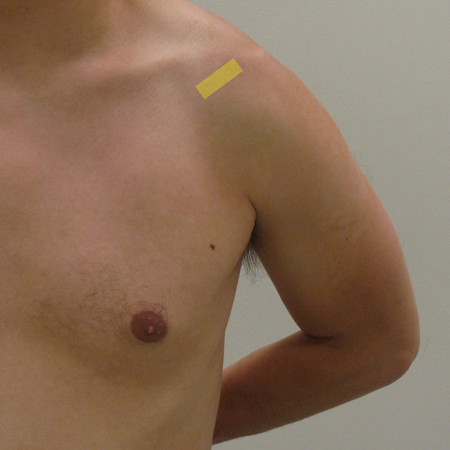
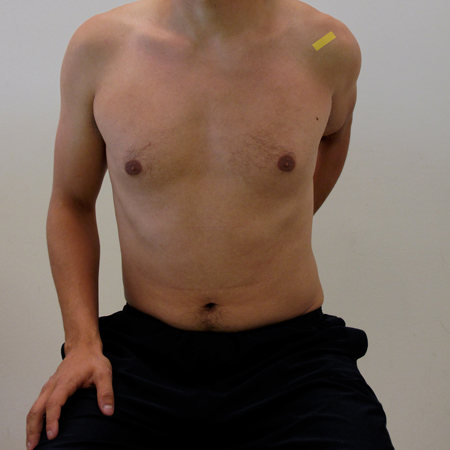
The position we will ask the patient to adopt will depend on the condition of his shoulder. If the patient feels pain, we will choose the position based on the severity, irritability and nature of the pain. The ultrasonographic evaluation may last a few minutes and the confort of the patient is of utmost importance.
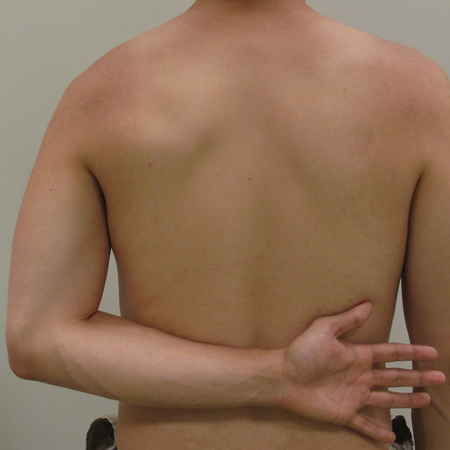
For a subject capable of placing the dorsal face of his hand in the middle of his back with little or no pain, we recommend the "Crass Position" (also called "Stress manoeuvre"
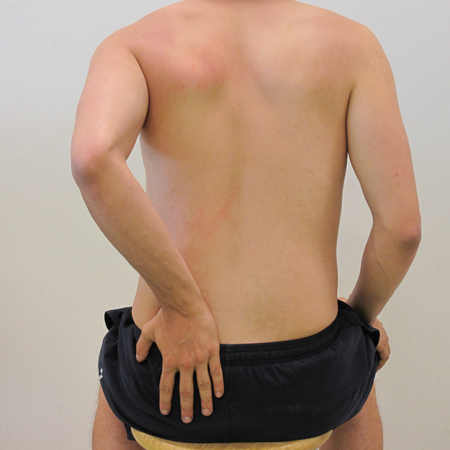
For a subject uncomfortable in the Crass position, we will choose the "Modified Crass Position" (also called the "Middleton Position")
Because the Crass position is often difficult to adopt, most authors recommend to adopt directly the modified Crass position.
Visualizing the orientation of the intra-articular portion of long biceps tendon is important because it is parallel to the path of the supraspinal tendon.
Place the probe in a longitudinal orientation at the bicipital groove as if you were evaluating the intra-articular portion of the long biceps tendon.
Turn the transducer so that the tendon of the long biceps appears as long as possible (ideally make sure the fibers are horizontal on the screen).
While maintaining the orientation of the probe, move the transducer up (cranial) and backwards in order to find the supraspinatus.
Gently oscillate the transducer while visualizing the tendon in order to avoid anisotropy.
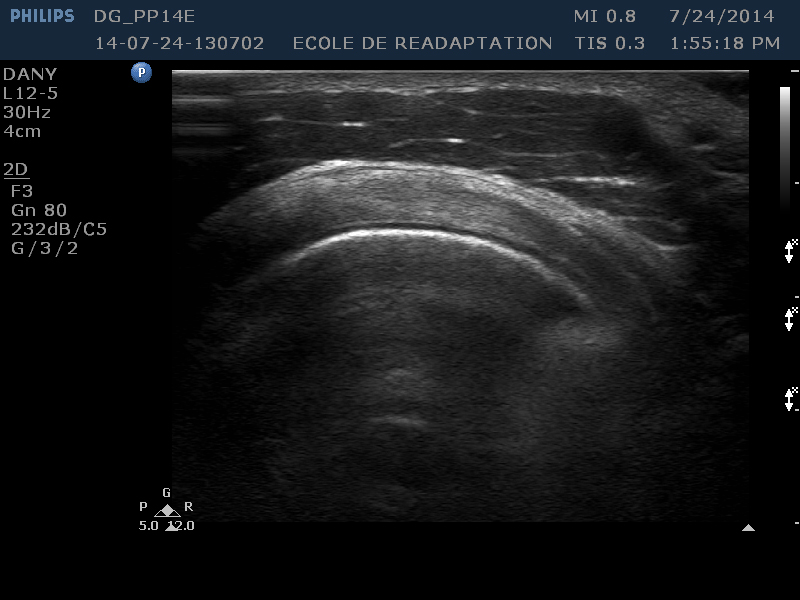
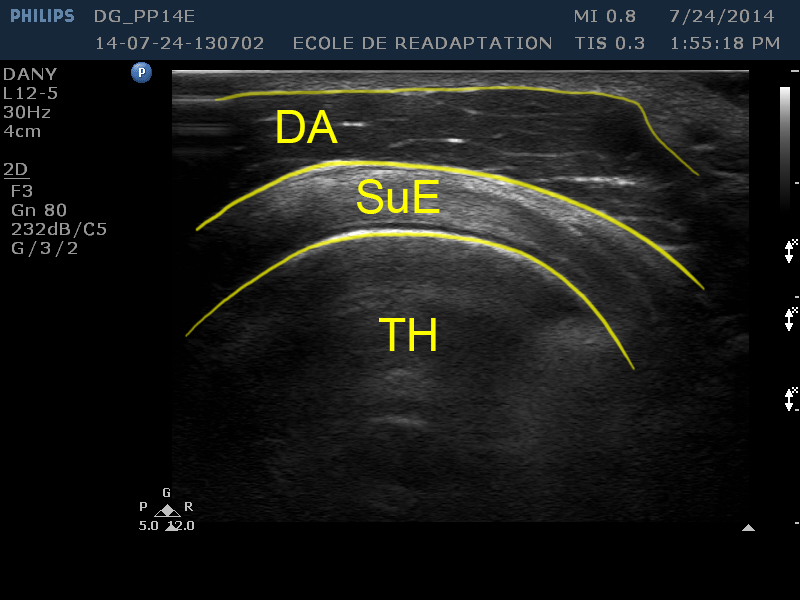
Identifying structures (on the screen) :
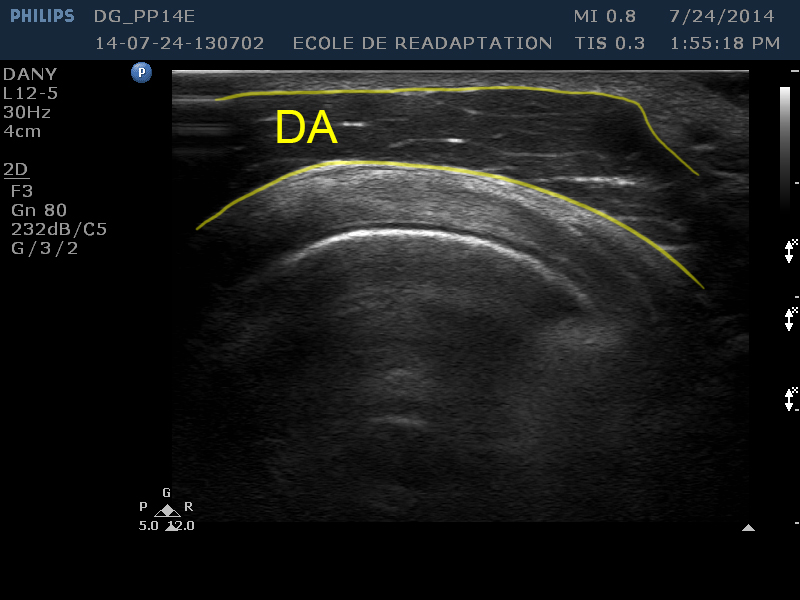
[AD]
The anterior deltoid appears at the top of the figure
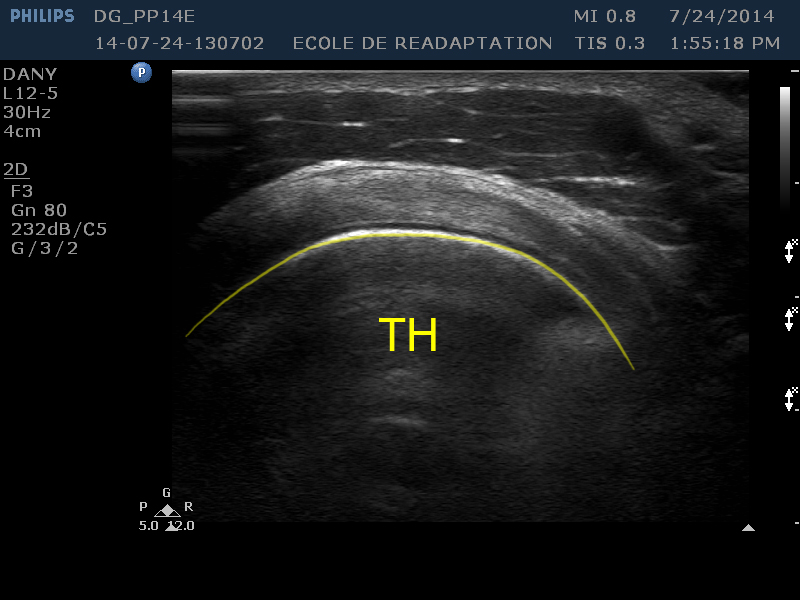
[HH]
The humeral head occupies the inferior half of the figure (hypoechoic zone)
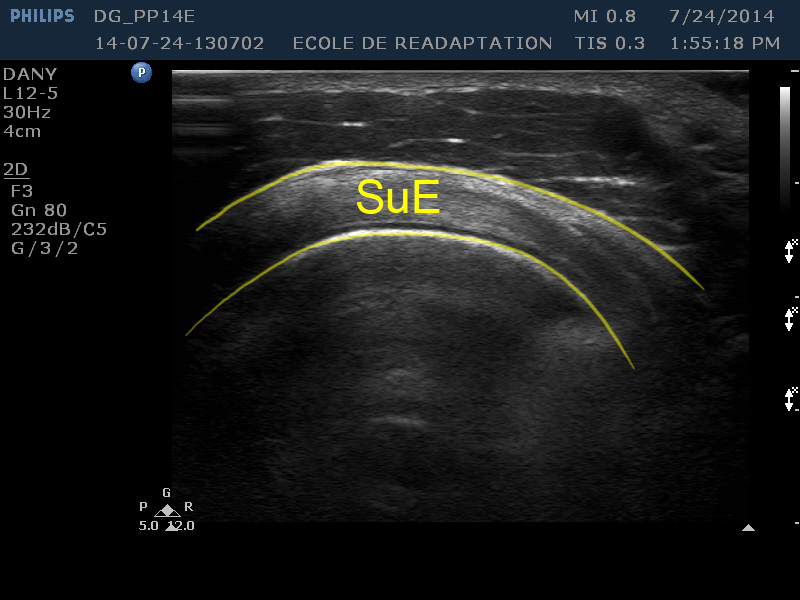
[SuE]
The supraspinal tendon appears as a long hyperechoic zone located between the anterior deltoid and the humeral head. The appearance of the the supraspinal tendon is sometimes compared to that of tire on a wheel (Jacobson)
The majority rotator cuff ruptures occur at the tendon of the supraspinatus tendon. In the worst rupture cases, the other tendons are also affected.
These ruptures are often associated to attrition and possibly to the concomitant presence of traumatic events. Irregularities in the cortical bone of the greater tuberosity can also be met.
Partial ruptures of the supraspinatus tendon can occur either at the surface adjacent to the bursa or near the articular surface.
A complete tear is when the tear of the tendon crosses from the articular surface to the bursa.
Most ruptures have an hypoechoic or anechoic appearance
Non-inflammatory tendinopathies or tendinosis give the tendon a hypoechoic and heterogene ultrasonographic appearance
********It is essential to be able to recognize when an image has anisotropy areas because these areas can reseemble the appearance of several phenonmeons such as tendinonse or even an ruptured tendon
often localized tendinosis often have that appearance.*****
The more diffuse tendinosis have their contours less defined and give the tendon an appearance close to that of an adjacent muscle.
**????????????Le muscle le plus touché Les tendinoses calcifiantes sont rencontrées, le plus souvent**
This is a sign suggesting a loss of tendinous fibers which involves generally a partial or complet rupture of the tendon.
In the case of a loss of volume it is possible to exclude the
presence of a tendinopathy because, on the contrary, tendinopathies are associated to a unchanged or increased volume of the tendon.